Having your child or teen tell you they want to die or finding your child lying on the floor after a suicide attempt are some of the most terrifying moments that parents can live through. Here at Bricolage, about 25% of the children and teens in our program enter after expressing thoughts of suicide or making an actual attempt.
While this is a terrifying moment as a parent, please realize that you are not alone. In Texas, suicide is the second leading cause of death for ages 10-24. Nearly 20% of Texas high schoolers have made a suicide plan and slightly over 12% have attempted it. That’s 1 in 10 high schoolers who have attempted suicide. That means that, of the 30 kids on the high school football team, 3 have possibly attempted suicide. Many families have been where you are now.
The above is certainly scary, but parents may find some comfort in the fact that only around 2% of children end up requiring medical attention after a suicide attempt and far fewer attempts result in an actual death. The vast majority of teens survive and, with the right support, go on to live normal and happy lives.
When our children express thoughts of suicide or make an actual attempt, we start to bombard ourselves with questions:
In this guide, we will provide answers to these and other questions.
In order to help our child, we have to understand the root causes of their suicidal thoughts. There is no one-size-fits-all answer here. Reasons for suicidal thoughts can be as unique as our children. However, there are often commonly identifiable drivers that we will explore below.
One of the first and most important things to keep in mind here is that almost everybody, at some time or another, has imagined killing themself. For most people, these are fleeting curiosities - looking over a cliff and wondering what it’d be like to jump off, having a horrible day at work and thinking about driving into a tree on the way home. Our minds are always exploring options and, for most people, when such a thought flashes through their head, they dismiss it immediately as nonsense.
In literature, Edgar Allen Poe explored this all-too-human tendency to think of things contrary to our own self-interest in his short story “The Imp of the Perverse.” The point is that, as disturbing as such thoughts can be, they’re quite normal and nothing to be overly concerned about most of the time.
However, these fleeting thoughts are not the ones that concern us. When our children come to us with thoughts of suicide, ideation has generally progressed from a fleeting thought to something much more serious.

There are many reasons for suicidal ideation to become stronger and one of those reasons is rumination. Neural pathways in our brains are strengthened by repeated thoughts and actions. The more we practice something, the better we get. Studying for a test helps us remember and recall information better. Hearing a song over and over again helps us memorize the lyrics.
In the same way, constantly thinking about suicide reinforces such thoughts and can also increase their frequency. Thoughts of suicide can be very scary. Instead of perceiving a sudden thought of killing oneself as their brain coming up with some random, perverse thought that gets dismissed right away, our children can begin to ruminate on it. Especially if they haven’t had such thoughts before, the emotional valence in their internal response can lead to increases in both the strength and frequency of such thoughts.
One strategy to help your child deal with thoughts of suicide is to sit down and openly discuss them. Let them know that everyone can have such thoughts at times and that that’s OK. Rather than ruminating on the thought, tell them to watch it appear in their mind’s eye, and then let it go and move on to something else.
Now, it’s very important here that we are not dismissive of our child’s thoughts. While helping them understand that such thoughts can be normal and that one strategy for dealing with them is to not dwell on them, if our child is coming to us in distress around such thoughts already, they have likely progressed to a severity where such a simple strategy is no longer enough. We want to listen attentively and take their concerns seriously at this stage.
When suicidal ideation has progressed to serious contemplation or higher frequency, there are often two primary reasons.
Pain is always hard to deal with, even as adults. For our children and teens, they have less experience with serious pain, both physical and psychological, and are less likely to have developed the coping skills to deal with it effectively.
Many children entering our program will state an end to pain as a primary reason for considering or attempting suicide. At this point, we need to discover the sources of their pain and then provide them with the tools to reduce or manage it.
This is where each child’s unique circumstances come into account. One child may be dealing with the loss of a loved one while another is being constantly bullied while another may be struggling with heavy drug use. Each of these situations can cause a lot of pain from which a child may want to escape.
In general, children start to view suicide as an option when they do not see any other options available to them. They have probably tried to solve the problem in various ways, but have been unsuccessful. As children with limited life experience, they can be unaware of options available to them and also are less likely to have dealt with extremely painful situations in the past, so do not have the perspective that “this too shall pass” like many adults.
By talking with them openly about the pain they’re experiencing, we can then help them explore potential solutions to either eliminate or reduce the pain, or learn to manage it. This could be learning to deal with stress, how to navigate online bullying, coping with feelings of anxiety or depression, etc.
Sometimes it’s just not possible to eliminate the source of pain, which is one way our kids can get stuck. For example, with the loss of a loved one, there is no way to change those circumstances, their loved one is gone forever. However, there are many ways to learn to live with grief and move past it. This could be doing something in their honor, journaling, identifying a goal the loved one had had for them and working towards it, leaning on others around them, etc.

When escape from pain is the goal, there should be a 3-step process in place to help your child:
The other most common reason for suicide is simply not wanting to live. This is frequently linked to a perceived lack of meaning and purpose. Your child may feel that their life doesn’t matter, that there is no reason for existing, or that nobody cares if they live or die.
It may even be a final attempt to exert meaning.”I’ll show them. Maybe when I’m gone, they’ll finally realize that I matter.”
Commonly, these feelings are strongly related to the child’s perception of relationships with others in their lives. They may feel that their existence doesn’t matter to others or that their existence is actually a burden to those around them. Humans are social creatures and our meaning and purpose often derives from the relationships we have with those around us. A study published in the JAMA found that longevity and well-being are strongly linked to a sense of meaning an purpose and that sense of meaning and purpose is often associated with helping or serving others, whether that’s family or the greater community.
Just like when exploring reasons for pain, discussing why they perceive a lack of meaning and purpose in their lives is essential to exploring solutions. Do they feel ignored by others, mistreated by others, uncertain about their future, unclear of their potential contributions to family or society? Answering these questions will start to give direction on how best to support your child.
Helping your child find a sense of meaning and purpose is often more difficult than addressing pain. Pain is usually easily identifiable, but finding a sense of meaning and purpose is often much more elusive.
To try to uncover this, talk to your child about their:
It can be helpful for your child to write these lists in a personal journal or somewhere they can refer back to often.
Reading books together can also be a way to explore this. These are best done as a family rather than asking your child to read or complete on their own. Here at Bricolage, we are a big fan of The Big Life Journal. Other books that can foster discussion and exploration are Chicken Soup for the Teenage Soul, The Purpose Driven Life (for families with a Christian background), A Man’s Search for Meaning, and Choose Life: Finding Meaning and Reasons to Stay Alive.
After exploring values, interests, relationships and other items listed above, the next step is to create two lists:
Reasons to stay alive may be things like, my brother cares for and needs me, or my family would be devastated if I died. Finding reasons to stay alive is helpul, but it’s also important to give children something to work towards. This could be volunteering in the community, succeeding in athletics, excelling in school, working towards a career, accomplishing a personal project, etc.
While striving to accomplish something is important in finding meaning in one’s life, we also want to help our child set achievable goals with realistic stepping stones. Large goals should be broken down into smaller goals. Sometimes those struggling with suicidal ideation also struggle with failure or self-confidence. Small wins are important. For example, if their large goal is to get an A in a certain class, then the first step would be turning their assignments in on time. If their current grade is a C, raising the grade to a B should be their next goal.

If goals are too large and seem too out of reach, then it’s easy to give in to failure and defeat, which will have the opposite impact to what we want. Identify the small wins, celebrate them, and then work towards the next step. In this way, goals become manageable and successes more frequent.
Sometimes children and teens do not know how to express their needs or feel that other methods have not worked. In these instances, a suicide attempt can be a cry for help, your teen saying, “I need help and I don’t know how else to ask for it.”
Addressing suicidal ideation or attempts for cries for help can often be as straightforward as ensuring your child feels heard and seen. One way to do this is to be intentional about family communication. This can seem very awkward at first, but establishing a weekly, or even daily, check-in to discuss the day and any feelings or concerns is one way to help your child feel seen and heard. This can even be done via video for family members who may live in different households or who travel often for work.
While less talked about, threats of suicide can also be a protest or an attempt to get their way. A child may threaten suicide or even act out an attempt in order to exert control on their environment. These situations can be incredibly difficult for parents to navigate. On the one hand, threatening suicide is not a negotiation strategy that anyone wants to condone. On the other hand, especially for teens who are willing to make good on their threats, the feelings of guilt that can occur after such an attempt can be very difficult to bear.
Somewhat fortunately, in these cases, your child doesn’t actually want to die. Though that can be a small consolation, especially if your child is willing to follow through on a threat to prove their point. Even though they may not actually want to die, mistakes can be made in any attempt, so such threats and actions need to be taken as seriously as for those children with such intentions.
In this situation, it’s just as important to have open discussions with your child and go through a Safety Plan. Particular emphasis should be placed on reasons why they want to live. There should be also very direct discussions of if they actually want to die or if they are looking for another outcome. They may say something like, “I’ll kill myself before letting you send me back to that school again.”
In circumstances like that, turn the discussion to their goal (not going back to that school) and what alternative options exist. Giving children realistic choices can be one way to allow them to exert control over their lives while remaining within feasible boundaries. For example, they could be given the option of going back to school or doing online schooling. They may state that they don’t want either option and they want to go to the private school nearby that costs $50,000 a year.
Here is an opportunity to discuss why that isn’t an option and redirect the conversation to the options that do exist. Open discussions are important throughout this process. Rather than simply state, “We can’t afford $50,000 a year for a private school”, have a frank discussion around family finances. Be open about what the family makes, what’s available, and what’s affordable. Then ask them if there is a way to make the private school work. Having them come to, and openly state the conclusion on their own, will help build buy-in.
Here’s an example of how a parent might frame the discussion at this point:
“After reviewing everything with us, you stated yourself that $50,000 a year for private school is not attainable for our family. So our options are returning to your current school or moving to online learning. I understand that neither choice is the perfect solution, but these are the options we have. We will support you in whichever option you choose. You don’t need to answer right now. Take some time to think about it, let’s discuss again tomorrow, and then let’s make a decision.”
It would then be helpful to discuss ways to communicate their desire for a particular outcome that doesn’t involve threats of any kind, suicide or otherwise. Sometimes, continuing planned family discussion times helps children feel heard while also giving them insight into why certain decisions are being made. One helpful tactic is, once all the circumstances around a decision are laid out, have them come up with and present options.
Maybe they want a new phone. After laying out costs, have them come up with ways to cover that cost. That’s an easier one. Maybe they want to hang out with a friend who’s a bad influence whom you don’t want them hanging out with. In that case, it’s about presenting other options and having them choose between them. An example framing could be, “Hanging out with Melissa is not an option we will agree to. You can choose to stay home, you can go with us to a movie, or you can choose a different friend and we’re happy to drop you off at their house on Saturday. Which one would you like to do?” If they refuse to choose one of those options, you can either tell them that you wil make the decision if they don’t, or you can ask them to present other options that don’t involve hanging with Melissa and which you are open to considering. In either instance, you’re giving them the control to make a decision within reasonable boundaries set by you as parents,
We get ideas from those around us, friends, family, the media. This is as true for suicide as it is for anything else. Research has confirmed the contagious nature of suicide. This research has shown that even teens hearing of a suicide of someone they know increases their likelihood of viewing suicide as a solution to their own problems, so it’s important to realize that when a suicide happens in the community, among family, or is being discussed in the media, suicide risk increases for any teen that’s exposed.
If a suicide is being widely reported, it’s almost impossible to shield your child from all such exposure. That would be an unrealistic goal. But reducing exposure can be helpful. If there is a famous suicide being reported in the news, make the decision to not turn on the news while your child is home until the news cycle moves onto something else.
Also, ALWAYS address news of a suicide that your child is exposed to. If the idea of suicide as an option is contagious, one might conclude that avoiding the topic altogether would reduce risk, but this is not the case. The cat is already out of the bag, so to speak, and it’s always better to have open communication channels than not.
Talk with your child about what they’ve heard, what they’re feeling, and also make sure to explore what other options are available to someone other than suicide. Check in with them frequently. One conversation often isn’t enough as a child’s feelings and thoughts can change over time or as exposure increases. This doesn’t mean every day needs to be a deep discussion; just a check-in with “Hey, remember that discussion we had the other day, just wanted to check in and see how your feeling. Anything changed or anything you want to talk with me about?” can be enough to keep communication channels open.
There are a number of factors that increase the risk of a suicide attempt among children and teens.
While no warning sign is conclusive in and of itself, parents need to be aware that sometimes only one warning sign is evidenced before an attempt. It’s also important to know that the more warning signs which are observed, the greater the risk. We recommend discussing any and all such warning signs with a professional such as a school guidance counselor or therapist. Also, many programs like Bricolage offer free psychological evaluations which include screening for suicidal ideation. You can always call us at 469 968 5700 to schedule a free evaluation for your child. While in person is strongly recommended, it is possible to do via video conference as well.
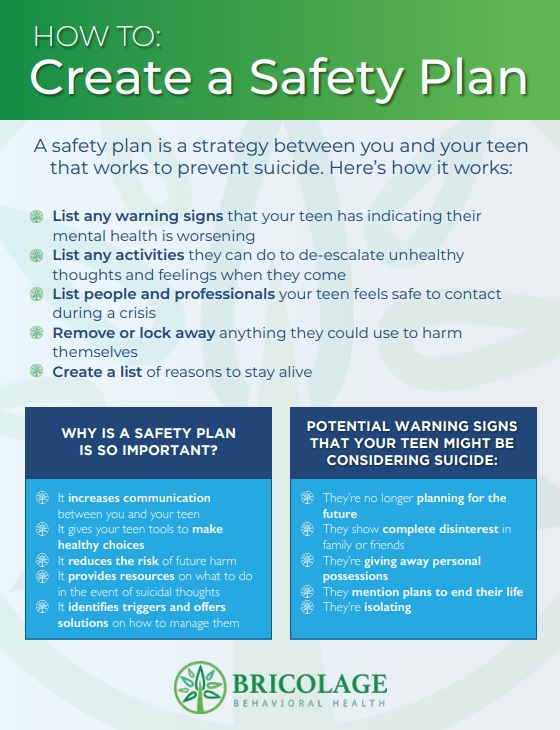
Major red flags prior to a suicide attempt are:
While most people who take or attempt to take their own lives display one or more warning signs, this is not always the case. Additionally, a single warning sign is not always clear or indicative of suicidal ideation. Children, especially teens, may use drugs, isolate, become aggressive, etc. for a plethora of reasons. Warning signs can be ambiguous or indicative of numerous underlying causes.
As parents, we want to know and be able to recognize warning signs, but we can’t blame ourselves for not seeing something. Engaging in preventative strategies such as maintaining open communication, doing frequent check-ins, and creating a safety plan are all helpful, but, in the end, we can’t control another’s behavior or see inside their minds. We may take all the precautions in the world and our child may still make an attempt. We can do our best and will continue to do our best for our children, but there are no guarantees in this life. However, be assured that if you engage in the preventative strategies outlined in this guide and you are able to recognize warning signs, it is highly likely that you’ll be able to have a positive impact on your child’s life and help them constructively deal with anything they are struggling with.
Sometimes we hear mental illness blamed for such behavior. So and so was depressed or anxious. While many who commit suicide are struggling with anxiety or depression, anxiety and depression are symptoms, not causes in and of themselves.
Why is our child depressed or anxious? It’s not uncommon to hear that mental health issues such as depression or anxiety are caused by chemical imbalances, bad genes, or faulty brain wiring, but, as we’ve discussed elsewhere, this is not the case. Depression, anxiety, and other mental health disorders are the responses to circumstances combined with an individual’s ability (or lack thereof) to cope with such circumstances.
As stated in the beginning, for the parent of a child who has attempted to kill themself, there is good news. According to the CDC, the majority of those who attempted suicide will not go on to die by suicide, meaning most people do not attempt again. Part of the reason for this is that prevention strategies are often effective. By following the information and using the tools in this guide, parents are equipped to be able to prevent a first attempt or another attempt.
Medications should always be an option to consider. While the mechanisms by which psychopharmaceuticals help in cases of suicidal ideation, depression, or anxiety are not yet well understood, about 40% of people report positive effects with their first antidepressant. However, effectiveness can vary drastically based on symptom severity, gender, age, and mental state.
In extremely simplified form, you can think of a psychopharmaceutical like other drugs. Pain killers don’t eliminate the source of pain, they simply depress our brain’s sensitivity to it. Cold medicines don’t cure colds, they suppress symptoms to make the cold more bearable.
Psychopharmaceuticals are not going to “cure” depression and anxiety or free one from suicidal thoughts, but they can help by suppressing or masking related thoughts and feelings. This is why medications are never the sole recommendation, but are always recommended alongside mental health counseling.
There is a popular myth that mental health disorders are caused by chemical imbalances in the brain, which medications can correct, but this is false. Instead, thought, behavior pattern, and environmental changes are essential to both short-term and long-term recovery.
In short, medications should always be explored as an option and part of the solution, but should never be viewed as the only component of a recovery plan.
There is no one-size fits all approach to therapy as it is dependent on the root causes of the disturbance, both the general ones outlined above and the specifics as to what’s driving your child’s negative thoughts and feelings. In therapy, we follow a particular sequence to identify root causes and then apply tailored interventions, mostly CPT and DBT discussed below, but other interventions are also possible depending on root causes.

Treating suicidality requires a three-pronged approach. Our children need to learn to restructure their suicidal thought patterns, deal with stressful and difficult situations in their lives, and take positive actions to address any issues driving their distress.
As always, we first need to discover WHY they are having suicidal thoughts. Common reasons given are:
Once we've determined why they are contemplating suicide, then we can start to address the causes.
Their why is the first step. We also need to understand related events, beliefs, and circumstances that contribute to the child's why. This is called a chain analysis. There is rarely one simple why. Instead, it’s a combination of multiple factors that we want to uncover. Here are some good questions to get started with a chain analysis:
Through the chain analysis, we want to discover the following:
Now that we understand the causes, addressing suicidal ideation requires thought pattern change, coping mechanisms, and action. For example, let’s take a common scenario where a child feels alone and unloved. We need to help the child do 3 things:
The action part is often forgotten in many interventions. A child who always feels like a failure needs help succeeding and celebrating small wins. A child who uses threats to get their way needs to be given positive communication tools to more effectively engage with others. Many struggling with suicidal thoughts lack feelings of agency. They feel they can’t or don’t have other options. By giving our children the skills to achieve desired outcomes, we empower them to find the solutions that work best for them.
Children can be empowered through the use of CPT or negative thought identification and restructuring techniques. CPT helps them rewire their thought patterns to focus on more life-affirming thoughts and on solutions rather than problems.
It’s also designed to help them find errors in their thinking. For example, asking a child who says they are unloved to recall a time a friend or family member told them they loved them, or a time when someone recently did something nice for them, indicating affection, empowers them to self-correct erroneous thoughts.
Here is a simple outline of a CPT process:
While that’s a short overview, if you want to get really into the use of CPT for suicidality, Kathleen Chard’s text on CPT for Suicidality is an excellent resource.
Elements of DBT are particularly helpful for patients dealing with suicidal thoughts due to its focus on emotional regulation and radical acceptance. The most important DBT skills for dealing with suicidal thoughts are:
Practicing the above CPT and DBT skills empower children to deal with disturbing thoughts as they arise and provides tools to help them regulate. DBT's focus on calmly analyzing and accepting situations before taking action is also directly relevant to managing strong emotional reactions.
For challenging maladaptive worldviews, the Improve, Pros/Cons, and Problem-solving skills are particularly relevant.
Different people prefer or excel with different tools, so it’s helpful to expose your teen to all of them. Once they have the tools that work well for them, then it’s time to practice, practice, practice.
In addition to the therapeutic techniques above, which may be challenging for someone not trained in such interventions, the below are some very straightforward actions any parent can take to help their child.

Here at Bricolage Behavioral, we know the pain, fear, and anxiety that can come from a child disclosing suicidal thoughts or an actual attempt. We’re here to help by provided structured day treatment and intensive teen therapies for intense issues. Contact us at 469-968-5700 to get started.
Bricolage Behavioral Health: Where Teen Minds Matter

Bricolage Behavioral Health is strength-based, skills-based, evidence-based, and medication-light. We empower your child or teen to develop the skills they need to take control of their mental health with effective, science-backed therapy.
At Bricolage Behavioral Health we believe that whole family healing affords your child the best chance for long term mental health and can put your loved ones on the path to a healthier, happier life.
Bricolage Behavioral Health
3204 Long Prairie Road
Suite A
Flower Mound, TX 75022
Mon - Fri: 8:30 AM–9:00 PM
Sat & Sun: 9:00 AM–5:00 PM
